
Digital Rural Health Corps
An AMSA program
An AMSA program
At every turn, we saw how AMSA's Digital Rural Health Corps could be a component of the work communities across the U.S. are already doing.
All 50 states have received first-year awards under the federal Rural Health Transformation Program, each tied to a state-authored plan to strengthen rural health. Rural workforce development and technology innovation are named strategic goals of the program. Digital access is among the priorities states have laid out. Telehealth, patient portals, remote monitoring: every tool assumes a patient who can navigate it.
We understand, from listening, that the barrier isn't just broadband access. It's navigability: the ability to understand, trust, and use what's been built. Older patients. Patients with lower health literacy. Patients who haven't had a reason to engage digitally before.
DRHC was built around two of those goals. Medical and pre-medical students deploy to rural communities, learn, train community trainers, and gather patient and community insights of a kind no state has had before. The data states and communities need to know what's actually working as they close the gap.
We put medical and pre-medical students into rural and underserved communities as Digital Health Navigators. They work with patients who self-identify as not digital health savvy. For many people, this is a first step, but an important one, into using the telehealth tools, patient portals, and remote monitoring devices their care now depends on.
DRHC plugs into the infrastructure a community already has, whether that's an AHEC network, a health system, a state agency, or an academic partner. No new layer to bolt on. IRB-approved patient and student data is generated along the way.
The learning runs both ways. Patients learn how to use the tools their care depends on. Students learn what rural care looks like from the patient's side, an experience that research shows increases the likelihood they'll practice rural medicine. The field gets a growing evidence base on the real barriers people face when trying to access care online.
DRHC isn't a curriculum. It isn't an app, a training, or a toolkit. It's all of those, deployed inside one operational framework that doesn't exist elsewhere.
We've looked. Telehealth training programs exist. Rural health electives exist. Community health worker programs exist. None of them integrate the elements that make DRHC work as a single, replicable system.
DRHC plugs into the infrastructure partners already have. It targets the right counties, not regions in the abstract. And the data it generates are built to feed state and national policy, not just academic publication. The five layers below show how.
The framework delivers in five layers.
The theory, model, logic, and outcomes framework. Written so a state director, a health-system or AHEC partner, an academic lead, or a funder can defend the program without being in the room when it was built.
The operational guide. Step by step, discovery through deployment through reporting.
Every instrument and material organized for immediate use: the FieldHub mobile app, the State Deployment Navigator, the training curriculum, scout reports, recruitment materials, and the reflection capture system.
Multi-site IRB template, IRB-approved eHEALS patient survey instrument, structured student reflection system, and the publication pathway through AMSA's open-access journal.
How your team gets operational and what continuing access looks like once you're live.
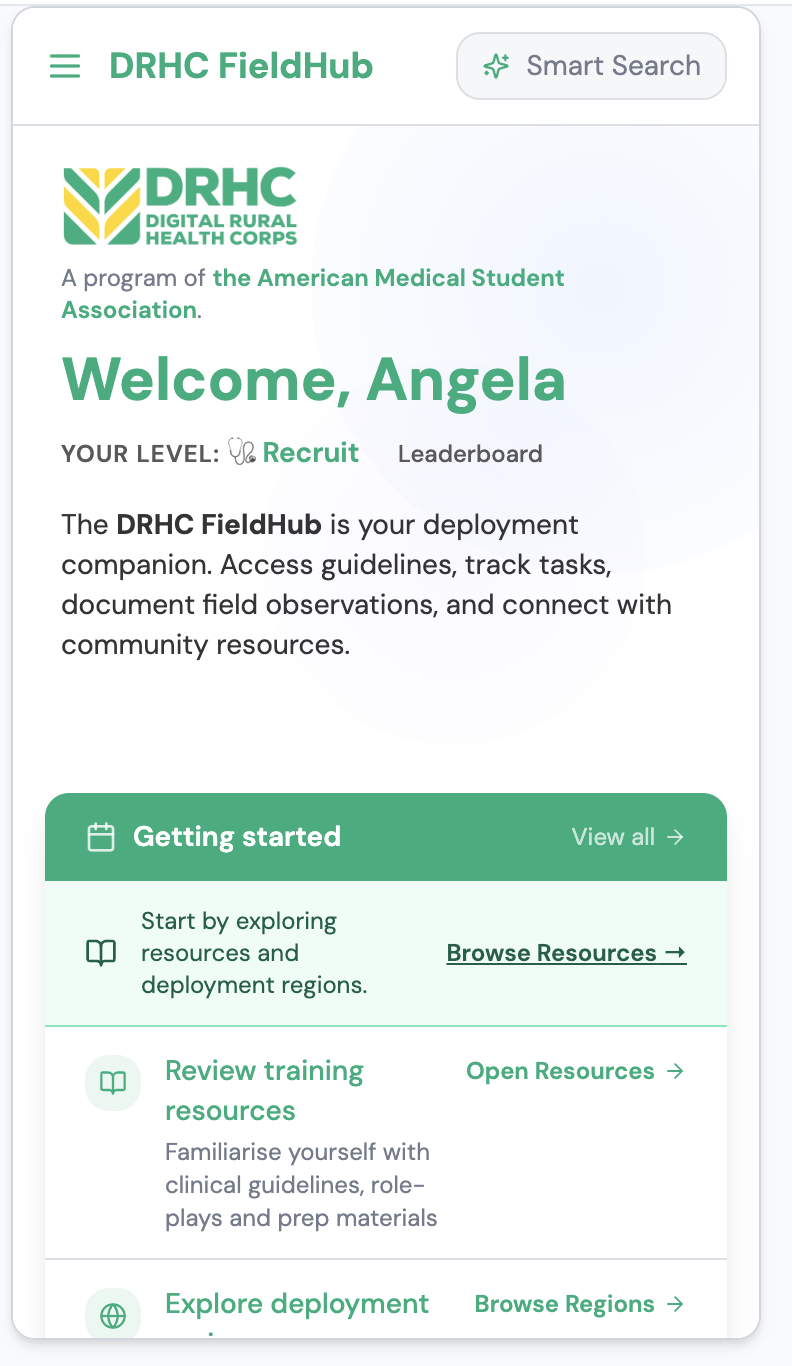
DRHC FieldHub · v1 · in field use
Every student navigator carries the same toolset into the field: protocols, scripts, encounter capture, and sponsor attribution in one place. Built for the realities of rural broadband and short patient windows.
The value isn't in the documents. It's in the system: the framework, the network, the data infrastructure, and the senior expertise to deploy it well and improve it over time. Partners don't buy a binder. They license access to a living program.
Every DRHC deployment moves through six phases. The Playbook documents each one in detail; this is the shape.
Structured workshop with your team. Priority counties, FQHCs, rural hospitals, health departments, deployment sites. In Georgia, this produced a map across six AHEC regions.
Students recruited from AMSA chapters and/or medical schools in your state or region. A 90-minute training session orients them to the framework, the FieldHub app, navigation protocols, and data collection. In person or virtual.
Trained students show up at their assigned sites as Digital Health Navigators. The FieldHub app guides their work and captures deployment data.
Patient survey data via the eHEALS instrument. Student reflections via a structured prompt system. Both streams preserved for analysis and research.
Deployment data becomes regional and state-level insights. Students with research interest get the AMSA publication pathway. Policy-relevant findings are documented and made available to your partners.
Deployment-specific learnings feed the next cycle. System-wide improvements get shared across the network.
Yours could be a good fit if you have deployment-partner capacity (AHEC, FQHC, health system, or academic) and a real digital access problem in your rural counties.
Year 1, we guide you through the framework adaptation, the platform onboarding, +. Year 2 and onward can take different paths, but at this point, you will have a foundation established, as well as data to help you guide what comes next.
Multiple partnership structures, from fully supported deployment through AHEC Scholars integration. We'll walk you through the process of determining which best suits your state.
We're raising for the layer that comes after a working pilot: the documentation, evaluation, and replication work that takes a model from "it works here" to "it scales across rural America."
Most rural digital health programs don't have IRB-approved patient and student data running through them. Ours does. That's the asset that makes DRHC credible to federal, state, and foundation funders thinking about evidence-based scale.
If you fund rural health, digital equity, physician workforce, or health-systems research, we'd like a conversation about where DRHC fits in your portfolio.
We'll send you a detailed DRHC Initiative Brief — a PDF you can share with colleagues, print, and mark up. Have a simple question? Drop it below and we'll respond within two business days — tops.
Founded in 1950, AMSA has shaped the way generations of US physicians practice medicine—and lead. Today it runs the national chapter network — the same network DRHC deploys through.